
The case management knowledge framework consists of what case managers need to know (knowledge, skills, and competencies) to effectively care for clients and their support systems. It includes two main elements:
- A nine-phase Case Management Process
- Six essential knowledge domains (previously seven domains that have been updated based on findings of the case manager’s role and function study that The Commission™ recently conducted)
These elements are applicable in any care or practice setting and for the various healthcare professionals who assume the case manager’s role and/or those directly or indirectly involved in the field.
Definition of Case Management
There are many definitions of case management. An Internet search for the definition of the term case management will result in thousands of references. Such results are confusing for case managers and others who are interested in case management practice. You may be unable to discern which definition is most credible or relevant.
Despite the large search outcome, experts would agree that there are no more than 20 or so definitions of case management considered appropriate. These definitions are available in peer-reviewed professional case management literature or on websites and in other formal documents of case management (or case management–related) organizations, societies, and government or nongovernment agencies.
The Case Management Knowledge Framework

So that you do not get confused as you read materials in The Commission's™ CMBOK®, the expert contributors who developed the case management knowledge framework in 2009 decided to use The Commission’s™ definition of case management available at that time to guide their work. (Note that the definition below has since been updated to reflect current appropriate information promulgated by The Commission™).
 “Case management is a dynamic process that assesses, plans, implements, coordinates, monitors, and evaluates to improve outcomes, experiences, and value.
“Case management is a dynamic process that assesses, plans, implements, coordinates, monitors, and evaluates to improve outcomes, experiences, and value.
The practice of case management is professional and collaborative, occurring in a variety of settings where medical care, mental health care, and social supports are delivered. Services are facilitated by diverse disciplines in conjunction with the care recipient and their support system.
In pursuit of health equity, priorities include identifying needs, ensuring appropriate access to resources/services, addressing social determinants of health, and facilitating safe care transitions. Professional case managers help navigate complex systems to achieve mutual goals, advocate for those they serve, and recognize personal dignity, autonomy, and the right to self-determination.” (Joint definition ACMA/The Commission, 2022)
Case Management Philosophy and Guiding Principles
Case management is a specialty practice within the health and human services profession. Everyone directly or indirectly involved in healthcare benefits when healthcare professionals and especially case managers appropriately manage, efficiently provide, and effectively execute a client’s care. The underlying guiding principles of case management services and practices of the CMBOK follow:
- Case management is not a profession unto itself. Rather, it is a cross-disciplinary and interdependent specialty practice.
- Case management is a means for improving clients’ health and promoting wellness and autonomy through advocacy, communication, education, identification of service resources, and facilitation of service.
- Case management is guided by the ethical principles of autonomy, beneficence, nonmaleficence, veracity, equity, and justice.
- Case managers come from different backgrounds within health and human services professions, including nursing, medicine, social work, rehabilitation counseling, workers’ compensation, and mental and behavioral health.
- The primary function of case managers is to advocate for clients/support systems. Case managers understand the importance of achieving quality outcomes for their clients and commit to the appropriate use of resources and empowerment of clients in a manner that is supportive and objective.
- Case managers’ first duty is to their clients – coordinating care that is safe, timely, effective, efficient, equitable, and client-centered.
- Case management services are offered according to the clients’ benefits as stipulated in their health insurance plans, where applicable.
- The Case Management Process is centered on clients/support systems. It is holistic in its handling of clients’ situations (e.g., addressing medical, physical, functional, emotional, financial, psychosocial, behavioral, spiritual, and other needs), as well as those of their support systems.
- The Case Management Process is adaptive to case managers’ practice settings and the settings where clients receive health and human services.
- Case managers approach the provision of case-managed health and human services in a collaborative manner. Professionals from within or across healthcare organizations (e.g., provider, employer, payor, and community agencies) and settings collaborate closely for the benefit of clients/support systems.
- The goals of case management are first and foremost focused on improving the client’s clinical, functional, emotional, and psychosocial status.
- The healthcare organizations for which case managers work may also benefit from case management services. They may realize lowered health claim costs (if payor-based), shorter lengths of stay (if acute care–based), or early return to work and reduced absenteeism (if employer-based).
- All stakeholders benefit when clients reach their optimum level of wellness, self-care management, and functional capability. These stakeholders include the clients themselves, their support systems, and the healthcare delivery systems, including the providers of care, the employers, and the various payor sources.
- Case management helps clients achieve wellness and autonomy through advocacy, comprehensive assessment, planning, communication, health education and engagement, resource management, service facilitation, and use of evidence-based guidelines or standards.
- Based on the cultural beliefs, values, and needs of clients/support systems and in collaboration with all service providers (both healthcare professionals and paraprofessionals), case managers link clients/support systems with appropriate providers of care and resources throughout the continuum of health and human services and across various care settings. They do so while ensuring that the care provided is safe, effective, client-centered, timely, efficient, and equitable. This approach achieves optimum value and desirable outcomes for all stakeholders.
- Case management services are optimized when offered in a climate that allows direct, open, and honest communication and collaboration among the case manager, the client/support system, the payor, the primary care provider (PCP), the specialty care provider (SCP), and all other service delivery professionals and paraprofessionals.
- Case managers enhance the case management services and their associated outcomes by maintaining clients’ privacy, confidentiality, health, and safety through advocacy and adherence to ethical, legal, accreditation, certification, and regulatory standards and guidelines, as appropriate to the practice setting.
- Case managers must possess the education, skills, knowledge, competencies, and experiences needed to effectively render appropriate, safe, and quality services to their clients/support systems.
- Case managers must demonstrate a sense of commitment and obligation to maintain current knowledge, skills, and competencies. They also must disseminate their practice innovations and findings from research activities to the case management community for the benefit of advancing the field of case management.
Principal Terms
Many terms in the CMBOK have multiple meanings, and you may be unclear about which meaning to apply. You might also not interpret the terms in the way the knowledge developers – who are case management experts – thought of them.
To get the most out of the knowledge these experts have shared in the CMBOK, take the time to review the following terms. Note that the literature may describe these terms somewhat differently; the descriptions shared herein clarify their use throughout the CMBOK.
Principal Terms Used in the CMBOK
| Term | Description |
|---|---|
| Benefit programs | The sum of services offered by a health insurance plan, government agency, or employer to individuals based on some sort of an agreement between the parties (e.g., employer and employee). Benefits vary based on the plan and may include physician and hospital services, prescriptions, dental and vision care, workers’ compensation, long-term care, mental and behavioral health, disability and accidental death, counseling, and other therapies such as chiropractic care. |
| Benefits | The type of health and human services covered by a health insurance plan (sometimes referred to as health insurance benefits, health benefits, or benefits plan) and as agreed upon between an insurance company and an individual enrollee or participant. The term also refers to the amount payable by an insurance company to a claimant or beneficiary under the claimant’s specific coverage as stipulated in the health insurance plan. |
| Caregiver | The person responsible for caring for a client in the home setting and can be a family member, friend, volunteer, or an assigned healthcare professional. |
| Case manager | The health and human services professional responsible for coordinating the overall care delivered to an individual client or a group of clients, based on the client’s health or human services issues, needs, and interests. |
| Case management plan of care |
A comprehensive plan of care for an individual client that describes:
|
| Case Management Process |
The process through which case managers provide health and human services to clients/support systems. The process consists of several phases that are iterative, cyclical, and recursive rather than linear and that are applied until clients’ needs and interests are met. The phases of the process are:
|
| Case management program |
(Also referred to as case management department.) An organized approach to the provision of case management services to clients and their support systems. The program is usually described in terms of:
|
| Client |
The recipient of case management as well as health and human services. “This individual can be a patient, beneficiary, injured worker, claimant, enrollee, member, college student, resident, or health care consumer of any age group. In addition, [use of] the term client may also infer the inclusion of the client’s support [system]” (CMSA, 2016, p. 32). NOTE: In the CMBOK, the term client is sometimes intended to include the client’s support system. |
| Client’s support system |
The person or persons identified by each individual client to be directly or indirectly involved in the client’s care. It “may include biological relatives [family members], a spouse, a partner, friends, neighbors, colleagues, a health care proxy, or any individual who supports the client [caregivers, volunteers, and clergy or spiritual advisors]” (CMSA, 2016, p. 32). |
| Community services and resources | Healthcare programs that offer specific services and resources in a community-based environment as opposed to an institutional setting (i.e., outside the confines of healthcare facilities such as hospitals and nursing homes). These programs either are publicly or privately funded or are charitable in nature. |
| Health |
An individual’s physical, functional, mental, behavioral, emotional, psychosocial, and cognitive condition. It refers to the presence or absence of illness, disability, injury, or limitation that requires special management and resolution, including the use of health and human services-type interventions or resources. NOTE: Throughout the CMBOK, the term health implies all aspects of health as described in the principal term, reflecting a holistic view of the client’s condition or situation. |
| Health and human services continuum |
The range of care that matches the ongoing needs of clients as they are served over time by the Case Management Process and case managers. It includes the appropriate levels and types of care – health, medical, financial, legal, psychosocial, and behavioral – across one or more care settings. The levels of care vary in complexity and intensity of healthcare services and resources, including individual providers, organizations, and agencies. NOTE: Throughout the CMBOK, the term healthcare refers to and incorporates “health and human services,” reflecting the broader community of professionals who serve clients and the continuum of services they provide. |
| Knowledge domain | A collection of information topics associated with health and human services and related subjects. These topics are organized around common themes (domains) to form high-level/abstract concepts that are considered to be essential for effective and competent performance of case managers. Examples of case management knowledge domains are Quality and Outcomes Evaluation and Measurement, and Care Delivery and Reimbursement Methods. |
| Level of care | The intensity and effort of health and human services and care activities required to diagnose, treat, preserve, or maintain clients’ health. Level of care may vary from least to most complex, least to most intense, or prevention and wellness to acute care and services. |
| Community services and resources | Healthcare programs that offer specific services and resources in a community-based environment as opposed to an institutional setting (i.e., outside the confines of healthcare facilities such as hospitals and nursing homes). These programs either are publicly or privately funded or are charitable in nature. |
| Payor | The person, agency, or organization that assumes responsibility for funding the health and human services and resources consumed by a client. Payors may be clients themselves, a member of the client’s support system, an employer, a government benefit program (e.g., Medicare, Medicaid, or TriCare), a commercial insurance agency, or a charitable organization. |
| Practice setting |
(Also referred to as practice site, care setting, or work setting.) The organization or agency at which case managers are employed and execute their roles and responsibilities. The practice of case management extends across all settings of the health and human services continuum. These may include, but are not limited to, payor, provider, government, employer, community, independent/private, workers’ compensation, or a client’s home environment. |
| Professional discipline | Case managers’ formal education, training, and specialization or professional background that is necessary and prerequisite for consideration as health and human services practitioners. Also refers to the professional background – such as nursing, medicine, social work, or rehabilitation – that case managers bring with them into the practice of case management. |
| Services |
Interventions, medical treatments, diagnostics, and other activities implemented to manage clients’ conditions, including health and human services issues and needs. The types of services implemented can be found in an individual client’s case management plan of care, medical treatment plan, or other related documents as applicable to the healthcare setting and the professional discipline of the provider of care and services. NOTE: The term services is used generically in the CMBOK to include the various types of care and services described above. |
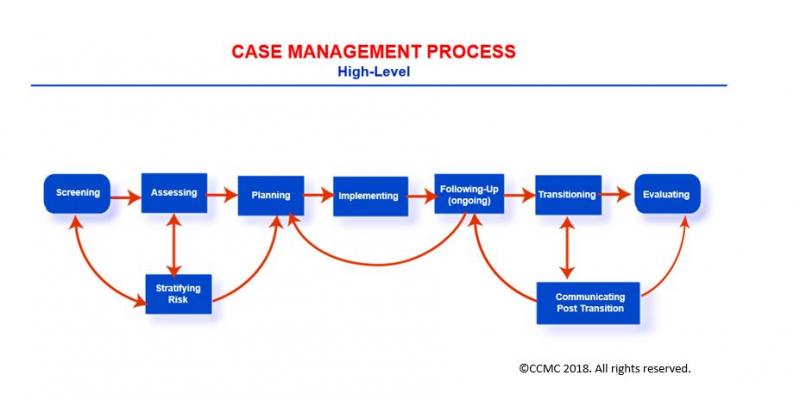
The Case Management Process
The Case Management Process consists of nine phases through which case managers provide care to their clients: Screening, Assessing, Stratifying Risk, Planning, Implementing (Care Coordination), Following-Up, Transitioning (Transitional Care), Communicating Post Transition, and Evaluating. The overall process is iterative, nonlinear, and cyclical, its phases being revisited as necessary until the desired outcome is achieved.
Centering on a client and the client’s support system, the Case Management Process is holistic in its approach to the management of the client’s situation and that of the client’s support system. It is adaptive both to the case manager’s practice setting and to the healthcare setting in which the client receives services.
The High-Level Case Management Process
Case managers navigate the phases of the process with careful consideration of the client’s cultural beliefs, interests, wishes, needs, and values. By following the steps, they help clients/support systems to:
- Evaluate and understand the care options available to them
- Agree on their care goals and priorities
- Determine what is best to meet their needs
- Institute action to achieve their goals and meet their interests/expectations
At the same time, case managers apply:
- Relevant state and federal laws
- Ethical principles and standards such as The Commission’s Code of Professional Conduct for Case Managers with Standards, Rules, Procedures, and Penalties (The Commission, 2023), which applies to persons holding the CCM® credential
- Accreditation and regulatory standards
- Standards of care and practice such as the CMSA Standards of Practice for Case Management (CMSA, 2022)
- Evidence-based care or practice guidelines
- Health insurance plan requirements and obligations, as appropriate
And at every phase of the Case Management Process, case managers provide vital documentation.
Client Source
Before looking more closely at the phases of the Case Management Process, first consider what triggers the process. You begin with the identification of a client. Without a client found to be in need of case management services, you have no need to launch the Case Management Process.
The client source – that is, how you, as case managers, come in contact with clients and/or their support systems – varies based on your practice setting.
Examples of Client Sources
| Care/Practice Setting | Highlights |
|---|---|
| Payor-based case manager | May implement the Case Management Process for a client upon direct contact via the telephone by the client/support system or upon referral from other professionals working for the payor organization such as a medical director, a claims adjuster, a clerical person, or a quality/performance improvement specialist. |
| Acute care setting–based case manager | May implement the Case Management Process for a client after referral from any of the healthcare team members, including the physician, primary nurse, social worker, consultant, specialist, therapist, dietitian, or manager.
In some organizations, case managers may visit every new admission and conduct a high-level review of the client’s situation for the purpose of identifying whether the client would benefit from case management services. |
| Community care setting–based case manager |
May implement the Case Management Process for a client after referral from the primary care provider or specialty care provider. In some instances, the case manager may initiate the process based on a request from the client/support system or based on a regulatory obligation such as health home requirement for Medicare or Medicaid beneficiaries participating in an accountable care organization or federally qualified healthcare center. |
| Vocational rehabilitation– or workers’ compensation–based case manager | May implement the Case Management Process for a client after referral from the acute- or community-based case manager or other healthcare providers who have identified the client would benefit from vocational rehabilitation case management services.
In some instances, an employer may refer a client (e.g., on-the-job injured worker) for vocational rehabilitation as part of the return-to-work plan of care. |
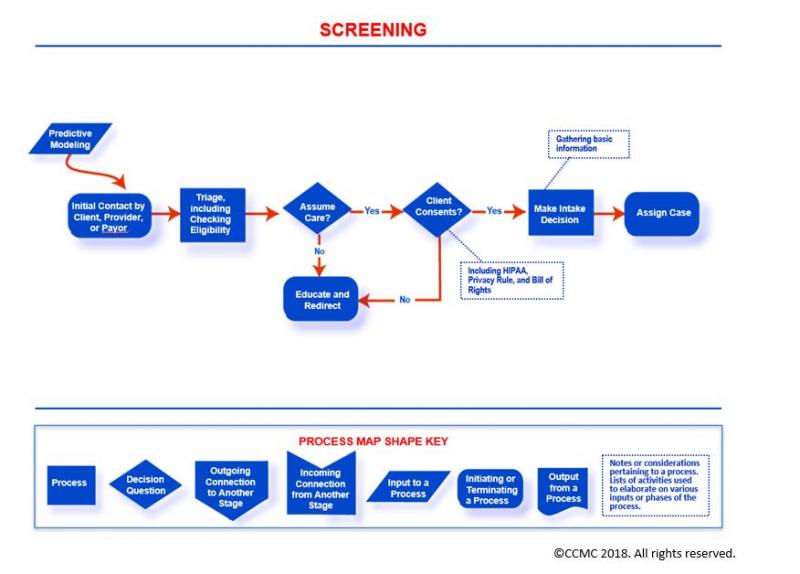
The Screening Phase
The Case Management Process: Screening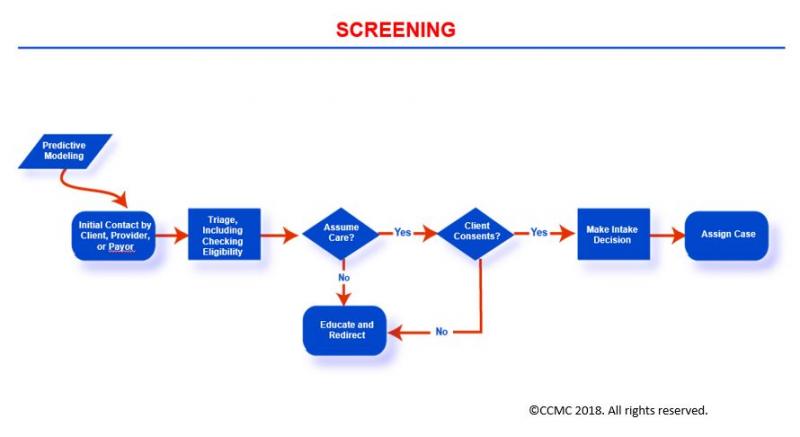
Click here to view map key for image
The Screening phase focuses on the review of key information related to an individual’s health situation in order to identify the need for health and human services (case management services). Your objective of the screening as the case manager is to determine if your client would benefit from such services.
Screening promotes early intervention and the achievement of desired outcomes. Key information about your client/support system you gather during screening may include the following (to the extent available):
- Risk stratification category or class
- Claims data
- Health services utilization
- Past and current health condition
- Socioeconomic and financial status
- Health insurance coverage
- Home environment
- Prior services
- Physical, emotional, and cognitive functioning
- Psychosocial network and support system
- Self-care ability
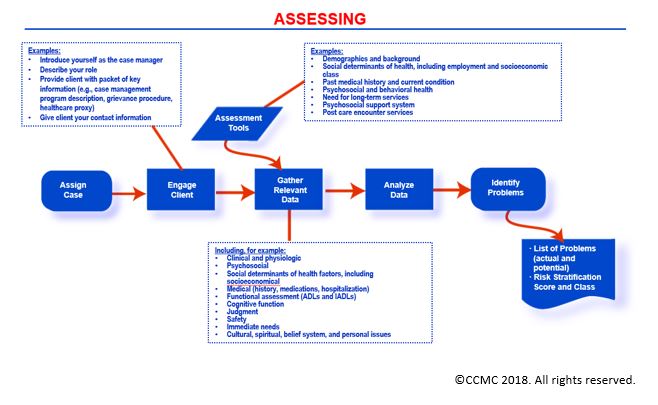
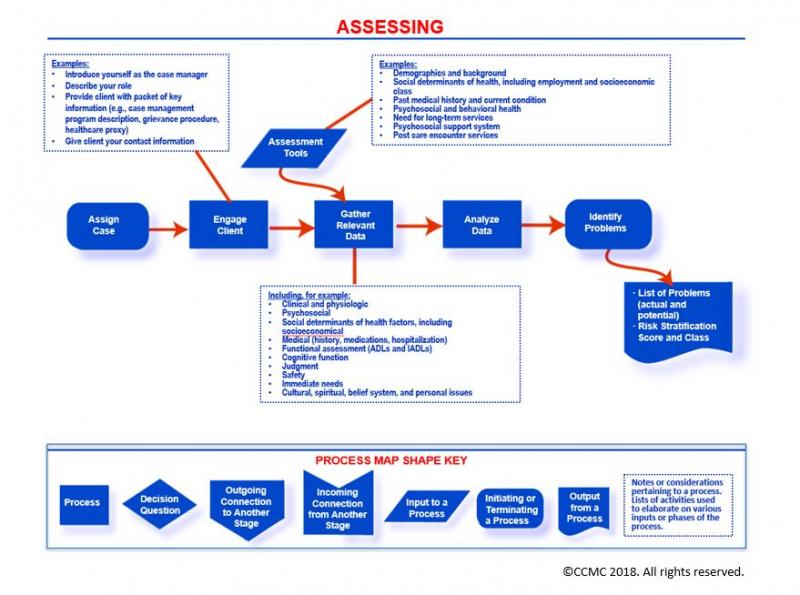
The Assessing Phase
The Case Management Process: Assessing
Click here to view map key for image
The Assessing phase involves the collection of information about a client's situation similar to those reviewed during Screening, however to greater depth. The information you collect about your client/support system may include:
- Past and current health conditions
- Service utilization
- Socioeconomic and financial status
- Health insurance plan benefits and coverage
- Home condition and safety
- Availability of prior services
- Physical, emotional, and cognitive functioning
- Psychosocial network and support system
- Health engagement
- Self-care knowledge and ability
- Readiness for change
You, as the case manager, have three primary objectives while assessing your client/support system:
- Identifying the client’s key problems to be addressed, as well as individual needs and interests
- Determining the expected care goals and target outcomes
- Developing a comprehensive case management plan of care that addresses these problems and needs while allowing you to achieve the care goals
You seek to confirm or update your client’s risk category based on the information you have gathered. You also may apply two key strategies for your effective information gathering. Using standardized assessment tools and checklists, you:
- Gather the essential information telephonically or through face-to-face contact with your client, the client’s support system, and the clinicians involved in your client’s care.
- Collect necessary information through a review of current and past medical records, personal health records if available, and communication with your client’s employer, health insurance plan representative, and others as you deem appropriate.
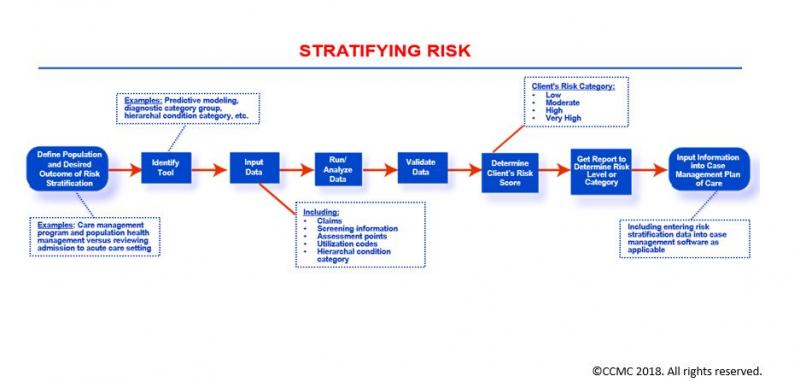
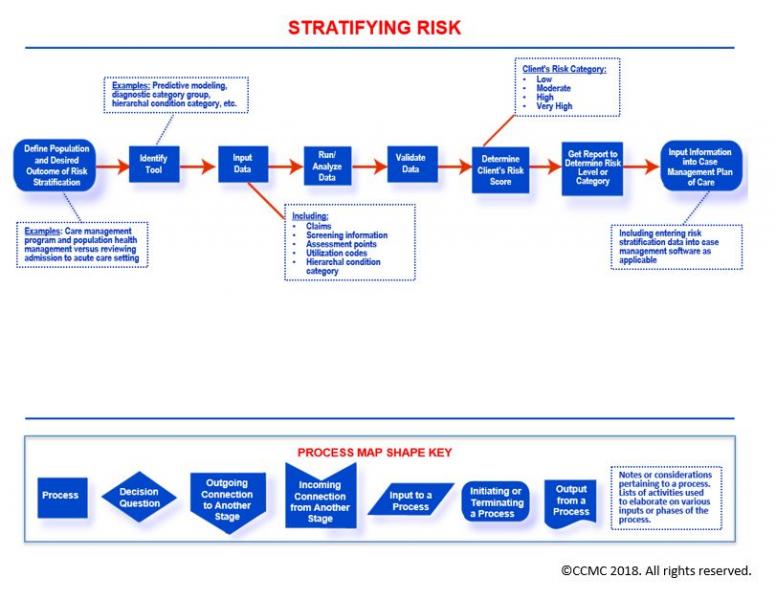
The Stratifying Risk Phase
The Case Management Process: Stratifying Risk
Click here to view map key for image
The Stratifying Risk phase involves the classification of your client into one of three risk categories – low, moderate, and high – in order to determine the appropriate level of intervention based on your client’s situation and interests. This classification allows you to implement targeted risk category–based interventions and treatments that enhance your client’s care interventions and outcomes.
When stratifying your client’s risk, as the case manager you complete a health risk assessment and biomedical screening based on specific risk factors for your client.
Factors applied in a client’s risk stratification may include:
- Presence and number of physical health conditions
- Medications intake: number and type (polypharmacy)
- Blood pressure
- Substance, alcohol, or tobacco use
- Nutrition and exercise habits
- Blood sugar level and lipids/cholesterol profile
- Emotional, mental, and behavioral health
- Access to care and utilization of healthcare services (e.g., emergency department visits or hospitalizations)
- Availability of psychosocial support system
- Gender, race, ethnicity, and age
- Socioeconomic and financial situation (e.g., limited income, no insurance, underinsurance)
- Other risk factors depending on the risk assessment tool/model applied
In some organizations, such as those that are payor-based, stratifying risks may take place prior to assessing the client. It also may be completed in an automated fashion using decision support systems and based on claims data. In such situations, you, as the case manager, review the automatically generated risk classifications and contact the client accordingly. You may also determine the need for contacting the client based on agreed upon and nationally recognized algorithms, criteria, and protocols.
It is common today to have a risk classification system that consists of four categories instead of three. The fourth and additional level refers to a small percentage of clients (i.e., no more than 3%) whose condition is extremely complex and requires an intensive amount of resources and the involvement of multiple healthcare providers with varied specialties. This group of patients is usually described as the “very high” risk category. When you are managing this category of clients, you provide comprehensive case management services while interacting with such clients at a frequency that exceeds once per month – as high as perhaps weekly.
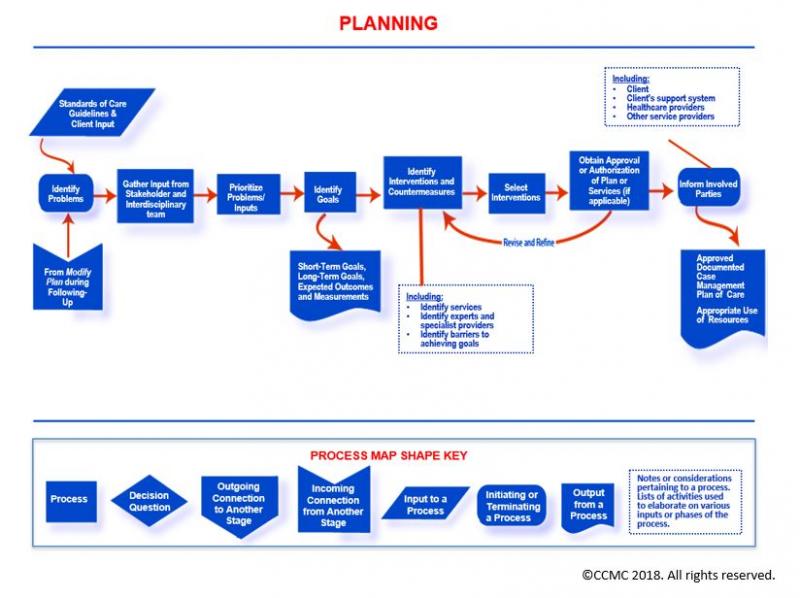
The Planning Phase
The Case Management Process: Planning
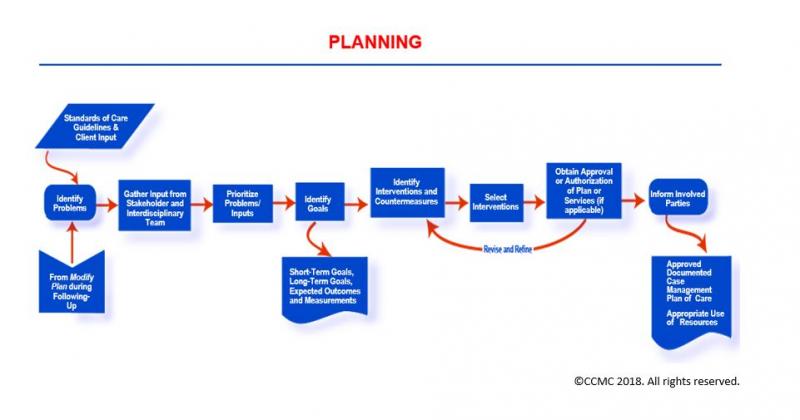
Click here to view map key for image
The Planning phase establishes specific objectives, care goals (short- and long-term), and actions (treatments and services) necessary to meet a client’s needs as identified during the Screening and Assessing phases.
You often consider the client’s risk classification or category in the design of the client’s plan of care.
During the Planning phase, you the case manager develop a case management plan of care for your client that considers inputs and approvals of the client/support system and the client’s healthcare providers. Your plan is action-oriented, time-specific, and multidisciplinary in nature. In this plan you address your client’s self-care management needs and care across the continuum, especially the services needed after a current episode of care; for example, home care services post hospital discharge.
In addition, the case management plan of care you develop identifies outcomes that are measurable and achievable within a manageable time frame and that apply evidenced-based standards and care guidelines. You finalize the Planning phase (i.e., development of a final case management plan of care for your client/support system) after you have received authorization for the health and human services from your client’s payor source and after the services and resources needed have been identified.
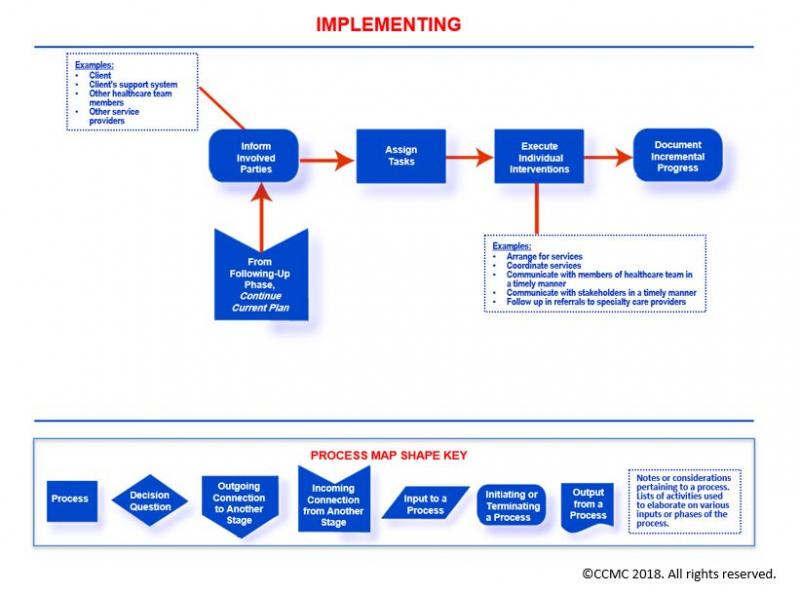
The Implementing (Care Coordination) Phase
The Case Management Process: Implementing (Care Coordination)
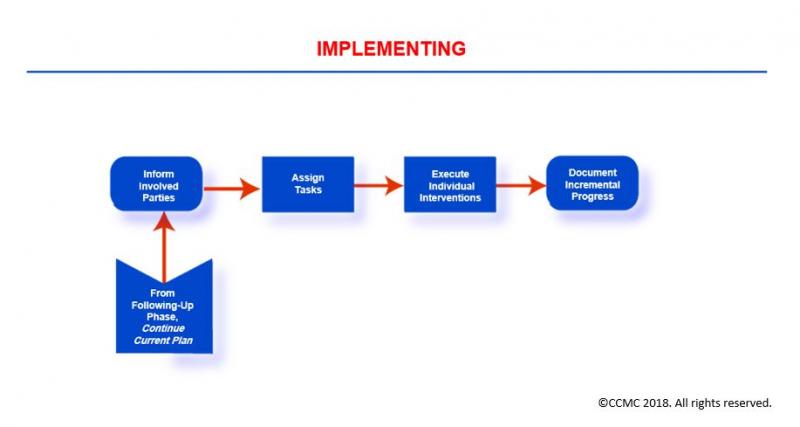
Click here to view map key for image
The Implementing phase centers on the execution of the specific case management activities and interventions that are necessary for accomplishing the goals set forth in your client’s case management plan of care. This is commonly known as care coordination.
During this phase, you the case manager organize, secure, integrate, and modify (as needed) the health and human services and resources necessary to meet your client’s needs and interests. You also share key information on an ongoing basis with your client and client’s support system, the healthcare providers/clinicians you are collaborating with, your client’s health insurance company/payor, and the representatives of community-based agencies you have engaged or will be engaging in the client’s care and case management plan.
The Following-Up Phase
The Case Management Process: Following-Up
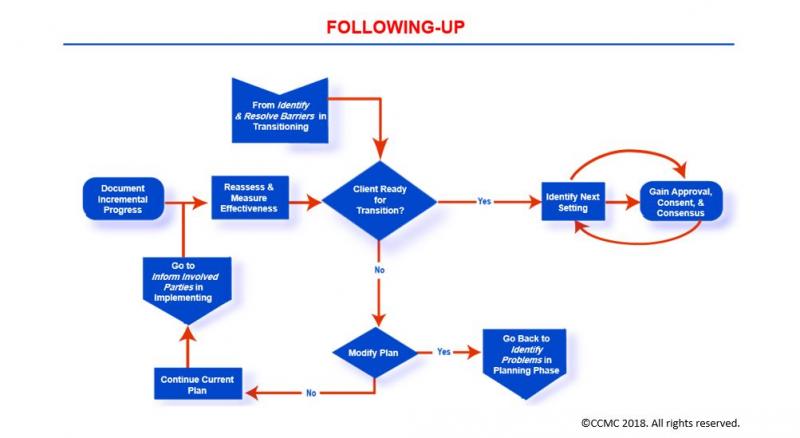
Click here to view map key for image
The Following-Up phase focuses on the review, evaluation, monitoring, and reassessment of a client’s health condition, needs, ability for self-care, knowledge of condition and treatment regimen, and outcomes of the implemented treatments and interventions. Here your primary objective is to evaluate the appropriateness and effectiveness of your client’s case management plan and its effect on your client’s health condition and care outcomes. During this phase, you:
- Gather sufficient information from all relevant sources.
- Share information with your client, client’s support system, healthcare providers, and others as appropriate.
- Document in your client’s health record the findings and modifications you may have made to your client’s case management plan, and recommendations for care.
- May repeat these activities at frequent intervals and as needed.
- Following-Up may indicate the need for a minor modification or a complete change in the case management plan of care. You use this phase as an opportunity to identify such needed revisions.
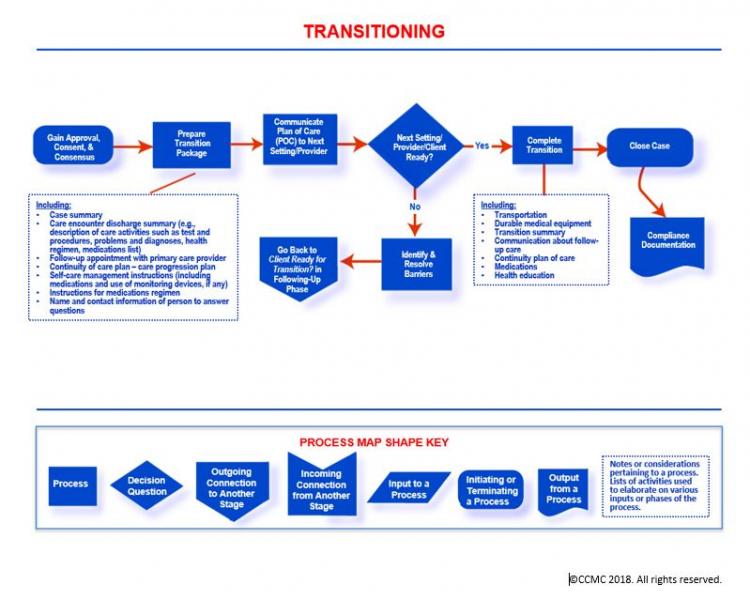
The Transitioning (Transitional Care) Phase
The Case Management Process: Transitioning (Transitional Care)
![]()
Click here to view map key for image
The Transitioning phase focuses on moving a client across the health and human services continuum or levels of care depending on the client’s health condition and the needed services/resources.
During this phase, you the case manager prepare your client and client’s support system either for discharge from the current care setting/facility to home or for transfer to another healthcare facility or a community-based clinician for further care. These activities are commonly known today as transitional care or transitions of care. In order to maintain continuity of care, you apply this phase’s activities to completely execute your client’s transition to the next level of care. You ensure your client’s safe transition through careful communication with key individuals (including sharing of necessary information) at the next level of care or setting, your client and client’s support system, and other members of the healthcare team.
Additionally, you may:
- Educate your client about post-transition care and needed follow-up
- Summarize what happened during an episode of care
- Secure durable medical equipment (e.g., glucose meter, scale, walker) and transportation services (if needed) for your client
- Communicate these services to your client, your client’s support system (such as caregiver), and to key individuals at the receiving facility or home care agency (if applicable) or those individuals assuming responsibility for your client’s care post transition
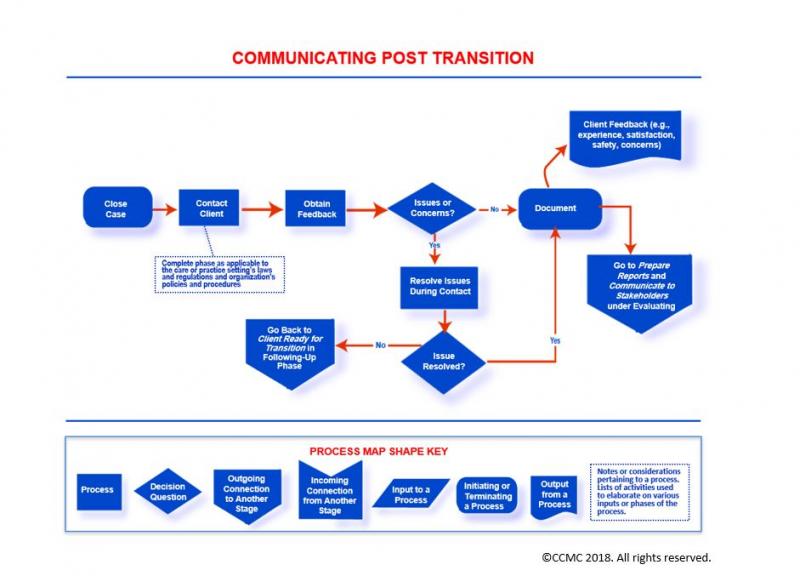
The Communicating Post Transition Phase
The Case Management Process: Communicating Post Transition
![]()
Click here to view map key for image
The Communicating Post Transition phase involves communicating with a client/support system for the purpose of checking on how things are going post transition from an episode of care.
As the case manager during this phase, you inquire about your client’s comfort with self-care, medications intake, availability of the post-transition services you may have arranged for (e.g., visiting nurse services), and presence of any issues or concerns. You also may solicit feedback regarding your client’s experience and satisfaction with services during the care episode.
During this phase, you:
- Follow up on the issues and problems you identify during the post-transition communication
- Seek resolution for the issues you identify
- Depending on the issue or concern you have identified, you may engage other healthcare professionals to reach resolution
- Report the feedback you gather during the communication to key stakeholders such as payors and providers of care
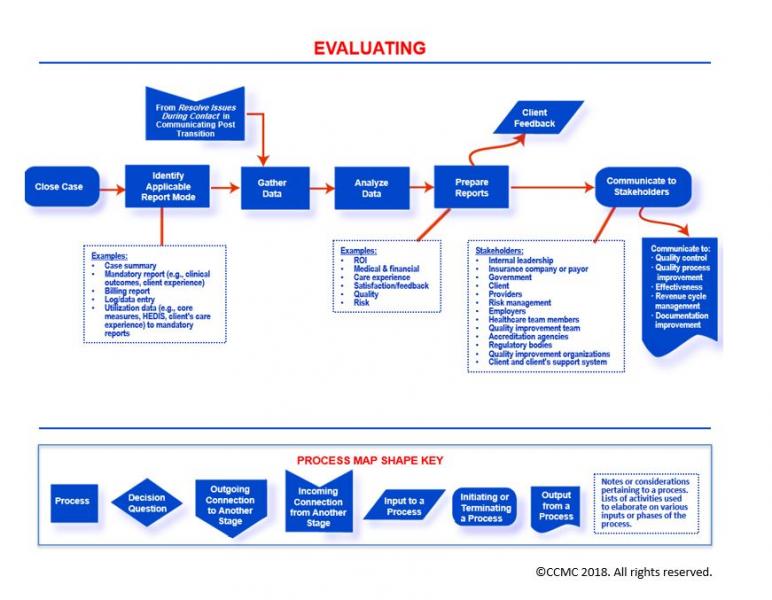
The Evaluating Phase
The Case Management Process: Evaluating
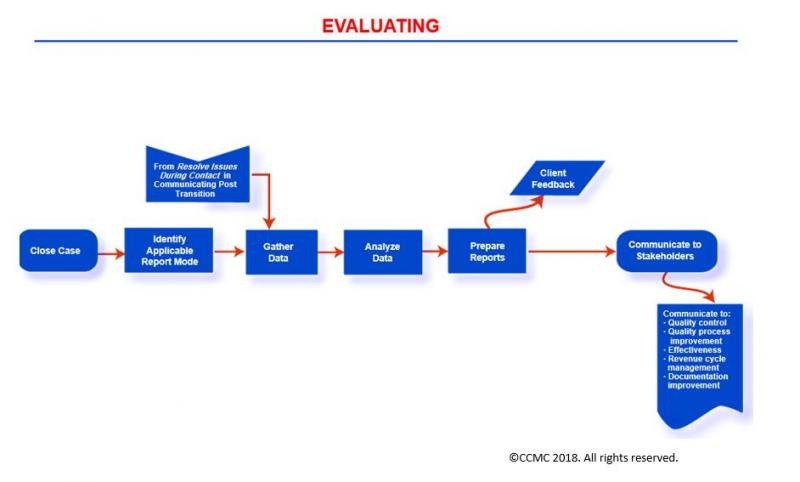
Click here to view map key for image
The Evaluating phase calls for measuring the results of implementing the client’s case management plan of care (e.g., the objectives, goals, treatments and interventions, and return on investment) and their effect on a client’s condition. In this evaluation, you focus on several types of outcomes of care:
- Clinical
- Financial
- Quality of life
- Experience and satisfaction with care
- Physical functioning
- Psychosocial and emotional well-being
- Self-care management ability and health engagement
- Knowledge of health condition and plan of care, including medications management
During this phase, you the case manager generate outcomes reports such as case summary, quality, cost/billing, satisfaction, outcomes, cost-benefit analysis, and return on investment. You also communicate the findings or disseminate the reports to key stakeholders such as government agencies (e.g., Centers for Medicare & Medicaid Services), the leadership team, client, payor, providers of care, employers, interdisciplinary team members, risk management staff, quality improvement team members, and others as deemed appropriate.
Essential Domains of Case Management Knowledge
Although case managers practice in a variety of care settings and are from varied backgrounds, The Commission™ has now defined six essential knowledge domains that encompass the realm of case management work and that apply to all care settings, health disciplines, and professional backgrounds. Each domain is further organized into subdomains.
The Six Essential Knowledge Domains and Subdomains
| Domain | Subdomains |
|---|---|
| Care Delivery and Reimbursement Methods |
|
| Psychosocial Concepts and Support Systems |
|
| Rehabilitation Concepts and Strategies |
|
| Ethical, Legal, and Practice Standards |
|
| Quality and Outcomes Evaluation and Measurement |
|
| Professional Development and Advancement |
|
Care Delivery and Reimbursement Methods
The Care Delivery and Reimbursement Methods domain consists of knowledge associated with the Case Management Process, systems of care provision, resources, and skills needed to ensure the effective and efficient delivery of safe, quality health and human services to clients/support systems. This domain also includes knowledge of reimbursement methods, funding sources, allocation of services and resources, and payor systems and concepts such as utilization review and management procedures.
Applying such knowledge in the execution of your role and responsibilities as case manager enhances your performance and improves your productivity, which then ultimately results in enhanced care outcomes for both your client and employer (healthcare organization) alike.
Success in your case manager’s role requires the work of a team: the client, the client’s support system, and the healthcare and service providers, including payor representatives and other clinicians.
The Case Management Team
© CCMC 2018. All rights reserved.
The Care Delivery and Reimbursement Methods domain also focuses on knowledge associated with case management administration and leadership, with program design and structure, with roles and responsibilities of case managers in various settings, and with skills of case managers (e.g., communication, problem-solving, conflict resolution, resilience, and others).
Additionally, knowledge in this domain is associated with various healthcare delivery systems and models across the continuum of health and human services and case managers’ practice settings. It includes knowledge of case management models, concepts, processes, services, and resources. Moreover, this domain addresses other topics such as levels of care, transitions of care, and collaboration among the various people involved in care such as the clients themselves, their support systems, multi-specialty care providers, community agencies, and payors.
Psychosocial Concepts and Support Systems
The Psychosocial Concepts and Support Systems domain consists of knowledge associated with the role clients’ cultures, values, beliefs, social networks, and support systems play in clients’ health and well-being, including health behavior and lifestyle. This domain also focuses on the impact of socioeconomic classes on clients’ health conditions, ability for self-care management, health engagement, health literacy and numeracy, and adherence to treatment regimen.
Additionally, this domain includes knowledge of the case manager’s role in addressing issues of underinsurance or lack of insurance, charity care, clients’ education regarding health condition and treatment options, counseling and psychosocial support, and clients’ home environments and living arrangements.
Rehabilitation Concepts and Strategies
The Rehabilitation Concepts and Strategies domain consists of knowledge associated with clients’ physical and occupational health and functioning, including catastrophic case management, workers’ compensation, vocational and disability concepts, strategies, and resources.
This domain also includes knowledge of life care planning, roles and skills of various healthcare providers in rehabilitation care settings, return-to-work concepts and strategies, types of rehabilitation settings/facilities, and use of assistive devices or durable medical equipment for rehabilitation and vocational purposes. In addition, this domain includes regulations pertaining to rehabilitation.
Quality and Outcomes Evaluation and Measurement
The Quality and Outcomes Evaluation and Measurement domain consists of knowledge associated with quality management, accreditation standards, care quality and safety, demonstrating return on investment, and cost-effectiveness. In addition, this domain includes demonstrating the value of case management, case load calculation, tools such as case management plans of care, and regulations related to case management.
Ethical, Legal, and Practice Standards
The Ethical, Legal, and Practice Standards domain consists of knowledge about the case manager’s role as client advocate and legal and ethical issues relevant to case management practice. This domain also focuses on:
- Codes of ethics and professional conduct for case managers
- Risk management
- Regulatory and legal requirements
- Ethical practices and principles
- Privacy and confidentiality
- Overall standards of case management practice
- Use of standards and guidelines in the management of clients’ care
- Strategies for ethical and legal practice
Professional Development and Advancement
The Professional Development and Advancement domain consists of knowledge associated with the roles and responsibilities of case managers in articulating, advancing, and demonstrating the value of case management practice. It also includes topics such as case managers’ involvement in scholarship activities (e.g., writing for publication, public speaking, research and utilization of evidence, training and education, and curriculum development), health or public policy work, accountability for ongoing education or learning, maintaining necessary skills and competencies for effective performance, engagement in practice innovation, and mentoring other case managers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}